

Introduction: Since 1990, Brazil has implemented a unified public health care, but access to specialized care remains a major challenge, especially due to delays in diagnosis and access to specialized centers. In order to help cancer care access, Hospital Israelita Albert Einstein, a private hospital, has implemented a public cancer clinic in Sao Paulo, only 11km apart. In an unprecedent situation in Sao Paulo, both public and private hospitals share most of the facilities, including laboratory, pathology, radiology, radiotherapy, pharmacy and medical team. Moreover, treatment protocols are the same and most drugs are also available in the public system. With 1 year of operation of the public clinic, we aim to analyze the outcome of patients with diffuse large B-cell lymphoma (DLBCL) compared with historical data from the private hospital. Moreover, since patients are only admitted after a confirmed cancer diagnosis, we aim to look at the impact of delayed diagnosis in the outcome of the patients.
Method: This is a retrospective study comparing the clinical features, treatment and outcome of patients with DLBCL treated in the public system with historical data from the private system. In order to minimize the impact of treatment protocols, only patients treated between January 2016 and February 2020 were used for historical comparison. All biopsies were reviewed by the same hemepathologist. Time to treatment initiation (TTI) time was defined by the number of days between biopsy and the first day of treatment cycle. Time from symptom onset to medical consultation (TSTC) was also calculated. Survival rates were estimated by Kaplan-Meier and differences assessed by log-rank test.
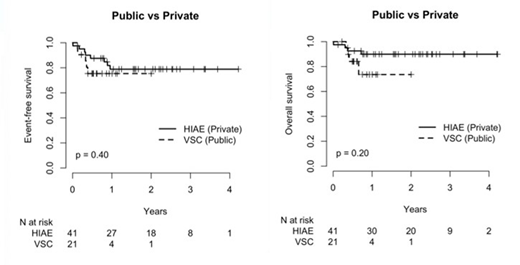
Results: In one year of operation, 23 patients with DLBCL were treated in the public clinic (PC) and were compared with 41 patients from the private hospital (PH), for a total of 64 patients. Clinical features were similar between PC and PH, and for all patients, median age was 61 years (range: 27-91), 76% with PS of 0-1, 78% with advanced stage and 45% with B-symptoms. Median R-IPI was 3 for both cohorts and approximately 50% of patients in both cohorts presented with R-IPI of 3 to 5. Interestingly, a difference in the cell-of-origin (COO) was observed between both cohorts, with a higher number of germinal center B-cell lymphoma in the PC (82% vs 52%, respectively, p=0.0041). TSTC was significantly higher in the PC compared to PH (160 vs 30 respectively, p<0.001), and it was mostly impacted by the delay in obtaining the biopsy result. Moreover, TTI was higher in the PC compared with PH (7 vs 39, respectively, p<0.0001) and was most impacted by the delay in receiving biopsy slides for review. With a median follow up of 18 months, 1 year-EFS was 76% and 1 year-OS was 86%for all cohort, with no statistical difference between public and private hospitals (p=0.40 and 0.20, respectively).
Conclusion: In our cohort of patients from public and private settings treated equally by the same resources, there was no difference in the outcome of patients. Despite TSTC and TTI were higher for patients from the public setting, no difference in survival was observed, and this may be partially explained by an enriched cohort of GCB DLBCL in the public system. The extremely low number of ABC DLBCL (4/23) is uncommon and suspicious for mortality of these patients before access to specialized care.
Perini:Janssen, Takeda: Honoraria; AbbVie, Janssen: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal